







A woman's eyes undergo changes during pregnancy, and it is necessary to know how to recognise physiological eye changes and differentiate them from the main pathologies that may arise in the pregnant woman.
Pregnancy implies a number of physiological changes essential to support and protect the foetus and prepare the woman for childbirth, these changes can affect all organs, including the eye. The changes that occur in pregnancy are usually transient, but occasionally they can become permanent.
Effects of pregnancy on the eye
In general, the effects of pregnancy on the ocular system can be divided into physiological changes and changes pathological.
Pathological changes can be further subdivided into:
- eye diseases already present before pregnancy and changing
- ocular complications of systemic diseases inherent to pregnancy.
Physiological changes
The most frequent physiological ocular change during gestation is theincreased pigmentation around the eyes. The brown discolouration of the face during this period is also called a gravid mask, chloasma or melasma, and is caused by increased levels of oestrogen, progesterone and melanotropic hormone (melanocyte-stimulating hormone).
Another frequently encountered condition is ptosisin which one or both upper eyelids are lowered compared to normal. Ptosis occurs in pregnancy generally in a unilateral form and is probably determined by the water retention and the hormonal changes.
A decrease in conjunctival capillaries and an increase in granularity in conjunctival venules may also occur during gestation.
Pregnancy can also affect the physiology of the tear film, resulting in thedry eye.
In pregnancy, specific causes of the onset of dry eye syndrome can be found in an increased immune reaction of the tear duct cells and the direct destruction of acinar cells by prolactin, transforming growth factor beta 1 (TGF-alpha1) and epidermal growth factor (EGF). The eye dryness can be further increased by dehydration due to nausea and vomiting.
Symptoms of dry eye can vary from mild to severe and include a burning sensation, itching and redness. Many patients also report a foreign body sensation in the eye, as if there were sand in it.
Other frequent symptoms include blurred vision, sensitivity to light and difficulty wearing contact lenses. In some cases, dry eye may cause excessive tearing as a reflex response to dryness.
The severity of symptoms may vary throughout the day and worsen in dry or windy environments. If left untreated, dry eye can lead to more serious conditions, such as eye infections and damage to the corneal surface.
During pregnancy one can also witness, especially in the final period, a reduction in corneal sensitivity. Changes in corneal curvature, oedema-related changes in corneal thickening and refractive index can occur. Changes in the cornea and tear system can also lead to contact lens intolerance.
Increased curvature of the crystalline lens can also cause a shift temporary myopicThis, like the conditions described above, generally resolves spontaneously after childbirth or after breastfeeding.
An important finding reported in numerous scientific works shows that during gestation the intraocular pressure (IOP) decreases by 19.6% in women with normal IOP and by 24.4% in those with ocular hypertension. Several mechanisms have been proposed to explain this reduction in IOP, including an increase in aqueous outflow, a reduction in episcleral venous pressure due to a decrease in systemic vascular resistance, reduced scleral rigidity as a result of increased tissue elasticity, and general acidosis inherent to the gestation period.
Contrasting works, finally, report changes in the visual field. The defects highlighted include concentric and bitemporal contraction, homonymous hemianopsia and central scotoma, and the mechanism proposed to explain the onset of these visual defects is based on the increased size of the pituitary gland, which would result in its abnormal anatomical relationship with the optic chiasm.
Pathological changes in the eyes during pregnancy
Diabetic Retinopathy (DR)
The number of women with diabetes in pregnancy is increasing due, in part, to the growing obesity of women of childbearing age. The diabetic retinopathy (DR) is the eye condition most commonly affected by pregnancy, and during this period there is an increased risk of disease development and progression.
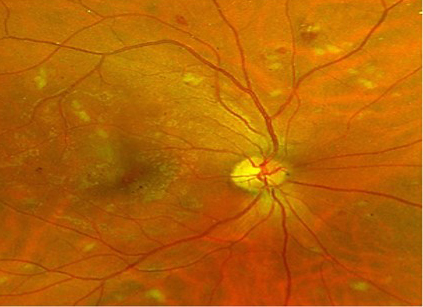 Several scientific studies have shown that up to 50% of the non-proliferative retinopathies may worsen at the beginning of pregnancy, then improving in most cases by the third trimester and/or post-partum. Factors influencing the progression of DR are the duration of diabetes, the degree of retinopathy at conception, glycaemic levels and the coexistence of vascular disease. Gestational diabetes, on the other hand, represents a very low risk for the development of retinopathy.
Several scientific studies have shown that up to 50% of the non-proliferative retinopathies may worsen at the beginning of pregnancy, then improving in most cases by the third trimester and/or post-partum. Factors influencing the progression of DR are the duration of diabetes, the degree of retinopathy at conception, glycaemic levels and the coexistence of vascular disease. Gestational diabetes, on the other hand, represents a very low risk for the development of retinopathy.
It is important to emphasise that the diabetic woman's ocular health status should be assessed and stabilised before pregnancy, and glycaemic control should be strictly maintained. It would also be advisable to carry out a complete eye examination at least every trimester and within three months after delivery.
Glaucoma
Women with pre-existing glaucoma may show improvement during pregnancy, however it is important to consult the ophthalmologist early in pregnancy so that the glaucoma can be closely monitored and all treatment options discussed with the patient.
Ocular complications of systemic diseases
Preeclampsia and Eclampsia
Preeclampsia, or gestosiseclampsia can occur after the 20th week of pregnancy and is characterised by the presence of one or more clinical signs such as oedema, proteinuria or hypertension. Eclampsia, on the other hand, is the most dreaded complication of pre-eclampsia, and is characterised by convulsions, mental confusion, headaches, nausea and vomiting, and can also cause severe fetal distress.
New diagnostic test
A new method is currently being developed based on an analysis of circulating free RNA (cfRNA) in maternal plasma, which, through a blood test carried out in the first trimester of pregnancy, will allow women at risk of developing pre-eclampsia to be accurately identified up to five months before clinical diagnosis.
So far, current screening tools, based on clinical risk factors or placental biomarkers, identify less than half of the cases and often do so when the disorder is already in progress.
Visual disturbances
Visual disturbances including scotoma, diplopia, decreased vision and photopsia were reported in 25% of women with severe pre-eclampsia and in 50% of women with eclampsia.
The changes in pre-eclampsia-related retinopathy are similar to those in hypertensive retinopathy, the most common finding being retinal arteriolar restriction, which is usually focal but may also be generalised. Other changes include retinal haemorrhage, oedema, exudate, nerve fibre infarcts and intravitreal haemorrhage secondary to neovascularisation.
There is a positive correlation between the severity of pre-eclampsia and the degree of retinopathy, the latter, however, generally resolves at the same time as the former. Cases of retinopathy due to pre-eclampsia may be more severe if there is co-presence of diabetes, chronic hypertension and renal disease.
Sheehan's Syndrome
Sheehan syndrome, or pituitary aplopexy, is a condition characterised by enlargement of the pituitary gland due to infarction or sudden haemorrhage in pituitary adenomas. Pregnancy is one of the risk factors for this condition, which can occur due to severe post-partum haemorrhage. This syndrome is considered potentially sight-threatening, as it can cause loss of vision (52%), visual field (64%) and/or ophthalmoplegia.
Graves' disease
Graves' disease is the most common cause (85%) of hyperthyroidism during pregnancy; there may be an exacerbation of the disease in the first trimester, which tends to improve in the second and third trimesters. It is very important to monitor the postnatal period closely, as sudden recurrences of the disease have often been reported. Treatment of pregnant women with Graves' disease should be multidisciplinary and involve an obstetrician for the management of maternal medical conditions, but also an endocrinologist to monitor thehyperthyroidism and a ophthalmologist to manage ocular complications. The repercussions of Graves' disease on the eyes are common and include: fixed gaze, delayed descent of the eyelids, proptosis and extra-ocular muscle paralysis.
Uveitis
The immunosuppressive effects and high levels of steroids in pregnant women can cause an improvement in uveitis especially in mid-gestation, although there is a risk of post-partum exacerbation. The management of patients with uveitis in pregnancy, therefore, may include a decrease in the administration of uveitis medication during gestation, so as to minimise side effects on the foetus, and after delivery an intensified follow-up to check for possible relapses.
On pregnancy and eye health
Diabetic retinopathy in pregnancy - Oculista Italiano
Pregnancy: how does it affect eyesight? - Italian Ophthalmologist
– Khawla Abu Samra. Oman J Ophthalmol. 2013 May-Aug; 6(2): 87-91
– Nursal Melda Yenerel and Raciha Beril Küçümen. Turk J Ophthalmol. 2015 Oct; 45(5): 213-219.
- Sushma Sharma, et al. The Obstetrician & Gynaecologist. Volume 8, Issue 3, Version of Record online: 24 JAN 2011.