






The situation in Italy and abroad.

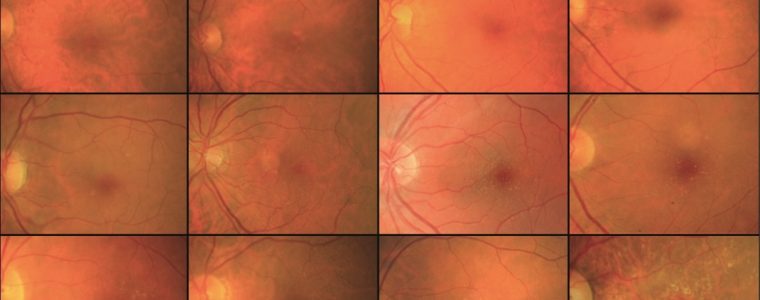
Zoster virus and herpes in the eye
For ophthalmologists theherpes in the eye caused by Zoster virus is a fearsome possibility, which moreover brings with it the risk of recurrences recurring.
Clinical studies on the frequency of herpes infection
The American study "Epidemiology of Herpes Zoster Ophthalmicus: Recurrence and Chronicity"published in Ophthalmology in 2016, confirmed recurrence rates of neuropathy from Herpes Zoster very high, close to 51%.
This figure is similar to that already reported by the Italian study 'Clinical features of ocular herpetic infection in an Italian referral centre', published in Cornea in 2014, which identified the most common manifestations of theherpetic infection the stromal keratitis and theuveitisfollowed by epithelial keratitis.
A recurrent infection
The severity of the ocular clinical picture and the fact that herpetic disease is not a 'single-stage' disease, but rather a recurrent infection can lead to chronic post-neuralgia pain. This eventuality makes it relevant for ophthalmologists and health authorities to promote the vaccination of populations against the zoster virus.
First of all, it should be remembered that zoster infection is so common because the virus, which is responsible for the childhood chickenpoxOnce contracted, it remains latent in the nerve cell bodies, without causing any symptoms.
Years or decades after a chickenpox infection, the virus can spread from one or more ganglia along the nerves of an affected segment and infect the corresponding dermatomere (an area of skin served by a spinal nerve), causing a painful rash.
The immune system under normal conditions is able to suppress the reactivation of the virus and prevent the reactivation of the herpetic infection, which is not the case in immuno-depressed patients and the elderly.
Eye symptoms
The eye is involved in about half of the cases of varicella-zoster virus reactivation along the V1 branch of the trigeminal nerve.
The ocular symptoms of shingles can be very severe and include a typical frontal skin rash (which is usually diagnostic) and unilateral painful inflammation of all tissues of the anterior and, rarely, posterior structures of the eye.
Therapy of herpetic infection consists of oral antiviral drugs, and usually topical mydriatics and corticosteroids.
Vaccine and shingles
A new recombinant vaccine has recently been formulated, which decreases the chance of contracting herpes zoster by approximately 97% in adults aged 50-69 years and 90% in adults≥70 years.
Vaccination is, therefore, recommended for immunocompetent adults ≥ 50 years of age, regardless of whether they have previously contracted herpes zoster or received the old live attenuated virus vaccine.
The recombinant zoster vaccine is administered in 2 doses of 0.5 mL each), 2 to 6 months apart.
For more information on the vaccine, see the study
Grupping K, et al. Immunogenicity and Safety of the HZ/su Adjuvanted Herpes Zoster Subunit Vaccine in Adults Previously Vaccinated With a Live Attenuated Herpes Zoster Vaccine. J Infect Dis. 2017 Dec 12;216(11):1343-1351. doi: 10.1093/infdis/jix482
Why vaccinate
The vaccine use would, first and foremost, be desirable for a number of concomitant reasons. Let us look at them analytically.
Extension of life expectancy
Firstly, throughout the developed world, there has been a progressive extension of average life expectancy and, therefore, an increase in the elderly component of the population, which is more likely to experience herpetic infection.
Frail patients
Secondly, the elderly tend to be more susceptible to zoster infection due to a number of age-related conditions such as immuno-senescence, to which can be added possible immuno-suppression from pharmacotherapy or diseases that compromise the immune system such as 'zoster'.AIDS.
Vaccination at a young age
It must be considered that varicella vaccination administered at a young age actually leads to less risk-exposure within the community, and therefore fewer infectious situations are present that would serve to maintain cell-mediated immunity.
The question of whether it is appropriate to vaccinate and at what age is quite complex.
When it is best to vaccinate
The study for the prevention of zoster (Shingles Prevention Study), published in 2005 in the New England Journal of Medicine first demonstrated the vaccine's safety and efficacy in reducing both the incidence of herpetic infection and the risk of postherpetic neuralgia.
United States
In the US until last year, the CDC (Centres for Disease Control) guideline was to recommend vaccination for patients of age over 60while the AAO and the American Society of Dermatology already recommended vaccinating patients over the age of 50.
Now as far as the US context is concerned, all recommendations have aligned, not least following the FDA's indication last October 2017, which endorsed the recommendation of vaccinate everyone over 50 against shingles.
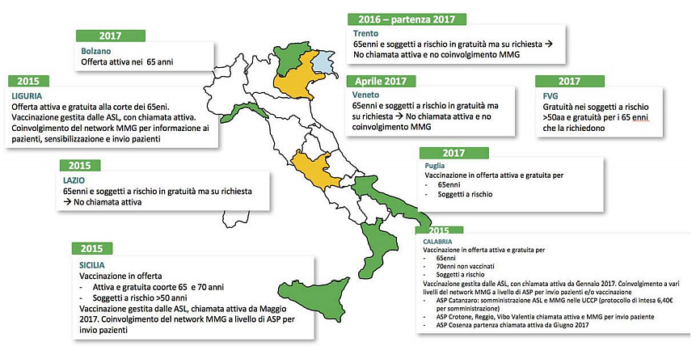
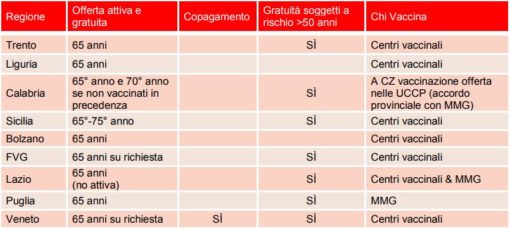
Situation Italy
As far as Italy is concerned, the National Vaccine Prevention Plan 2017-2019, included in the Livelli Essenziali d'Assistenza (LEA) (Essential Levels of Care), now recommends the vaccination of 65-year-olds.
In these cases, vaccination is free of charge and the picture summarises the situations in the different Italian regions.
- Tran KD, Falcone MM, Choi DS, et al. Epidemiology of Herpes Zoster Ophthalmicus: Recurrence and Chronicity. Ophthalmology. 2016 Jul; 123(7): 1469-1475.
- Miserocchi E, Fogliato G, Bianchi I, et al. Clinical features of ocular herpetic infection in an Italian referral centre. Cornea. 2014 Jun;33(6):565-70.
- Ministry of Health National vaccination prevention plan