






Ocular syphilis is quite rare, but can have a serious impact on the visual apparatus and, above all, is extremely difficult to diagnose correctly.

Introduction
Ocular syphilis is a rather rare but serious complication of untreated syphilis, a sexually transmitted bacterial infection.
Ocular syphilis can affect any part of the eye and can have a serious impact on the visual apparatus.
It is an extremely difficult condition to diagnose correctly, which can threaten vision if not diagnosed and treated in a timely manner.
Prevalence
Globally, there are about 12 million new cases of syphilis per year, of which about 55,400 occur in the United States. Ocular syphilis occurs in an estimated 1% to 5% of neurosyphilis cases in the United States.
Cause and characteristics of infection
Syphilis is an infection caused by the bacterium spirochete Treponema pallidum and can have severe ocular manifestations, likely involving all structures of the eye, leading to interstitial keratitis, chorioretinitis, retinitis, retinal vasculitis and neuropathy of the cranial nerves and optic nerve.
Patients with ocular syphilis are also at risk of neurosyphilis.
Syphilis is an infection transmitted mainly sexually, but also by contact with skin and mucous membranes, or trans-placental from mother to unborn child.
The spirochete Treponema pallidum, First identified in 1905 by Schaudinn and Hoffman, it penetrates through the skin and mucous membranes, reaches the lymph nodes and then spreads systemically.
Classification
It is possible to distinguish between a congenital (or transplacental) and an acquired form of this disease.
Acquired syphilis is characterised by three clinical phases - primary, secondary and tertiary - and involves numerous organs and systems.
Signs and symptoms
General signs and symptoms of syphilis may include:
- Red eyes.
- Myodesopsias.
- Pain in the eyes.
- Sensitivity to light (photophobia).
- Abnormal eye movements.
- Argyll-Robertson pupil, a term referring to the small pupils that become smaller (shrink) when focusing on a nearby object, but not when exposed to bright light.
- Blurred vision or loss of vision.
- Lesions (bumps or spots) on or in the eyes.
- Ulcer (painless sore) on the eyelid (rare).
Therapy and dissemination
Prior to the advent of penicillin, syphilis was associated with a high mortality and morbidity rate, but with the introduction of antibiotic therapy, coupled with changing socio-economic conditions and a reduction in risk behaviour, the incidence of syphilis declined rapidly.
In recent years, however, the disease seems to have regained strength, even in the higher-income social strata. In Italy, as far as the time trend is concerned, syphilis I-II cases remained stable until 2000, while thereafter they increased significantly. In 2005, in particular, there was a fivefold increase in diagnoses compared to 2000 and a new peak in 2016.
Eye involvement
Ocular involvement in syphilis is rare and typically occurs in secondary or tertiary syphilis.
Signs and symptoms
General signs and symptoms of syphilis may include:
- Red eyes.
- Myodesopsias.
- Pain in the eyes.
- Sensitivity to light (photophobia).
- Abnormal eye movements.
- Argyll-Robertson pupil, a term referring to the small pupils that become smaller (shrink) when focusing on a nearby object, but not when exposed to bright light.
- Blurred vision or loss of vision.
- Lesions (bumps or spots) on or in the eyes.
- Ulcer (painless sore) on the eyelid (rare).
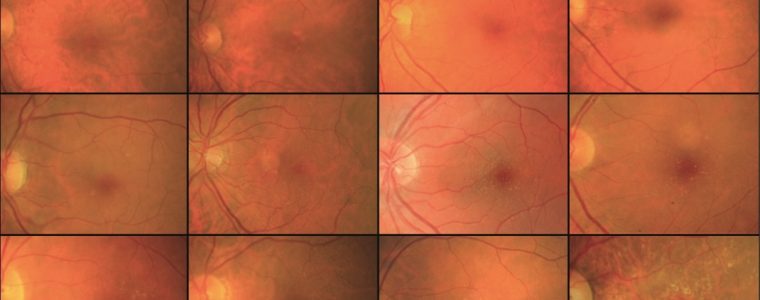
The most frequent ocular clinical manifestation is theuveitiswhich is found in the 2.5-5% of patients with the tertiary form of the disease.
The main signs include keratic precipitates, iritis and iridocyclitis, and the inflammation can occur in both granulomatous and non-granulomatous forms.
Less common are manifestations in the posterior segment, including vitritis, vasculitis, papillitis, exudative retinal detachment, uveal effusion, central retinal vein occlusion, neuroretinitis and retinal necrosis.
A sneaky pathology
Health professionals describe syphilis as 'the great copycat' because it can resemble many other diseases.
Syphilis is, in fact, a sneaky disease as it does not manifest itself with pathognomonic signs, but with a variety of signs and symptoms, making the clinical course complex, which can lead to a missed diagnosis or a delay in treatment.
Differential diagnosis
In syphilis, ocular involvement, and in particular at the level of the posterior segment, goes in differential diagnosis with other infectious diseases such as tuberculosis, or non-infectious diseases such as sarcoidosis, or other hereditary retinal diseases.
Recommended diagnostic pathway
The above highlights the extreme importance of performing systemic, serological and radiological investigations in all cases of papilla oedema or retinal changes without apparent cause, even in patients with a silent history of known infectious diseases.
Interdisciplinary team collaboration
Also crucial is the interdisciplinary collaboration between ophthalmologist, infectivologist, internist and neurologist for the management of suspected 'masquerade conditions' such as syphilis, which has always been referred to as the 'great masquerader', as it presents itself with a variety of systemic manifestations that can cause misdiagnosis.
See also:
- Ocular syphilis: increasing incidence globally - Oculista Italiano
- Ocular manifestations of dermatological diseases: infectious and inflammatory disorders - Oculista Italiano
- Update on uveitis (oculistaitaliano.it)
- Singh AE. Ocular and neurosyphilis: epidemiology and approach to management. Curr Opin Infect Dis. 2020 Feb;33(1):6672. doi: 10.1097/QCO.0000000000000617. PMID: 31789673.
- Trevelyan G, Kumar K, Russell GK, Wickremasinghe M. Secondary syphilis presenting with acute unilateral vision loss and a widespread maculopapular rash. BMJ Case Rep. 2019 Sep 18;12(9):e230341. doi: 10.1136/bcr-2019-230341. PMID: 31537590; PMCID: PMC6754640.
- Browning DJ. Posterior segment manifestations of active ocular syphilis, their response to a neurosyphilis regimen of penicillin therapy, and the influence of human immunodeficiency virus status on response. Ophthalmology. 2000 Nov;107(11):2015-23. doi: 10.1016/s0161-6420(00)00457-7. PMID: 11054325.